To date, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is the virus responsible for the coronavirus disease 2019 (COVID-19), has infected over 603 million individuals and claimed more than 6.4 million lives worldwide.
About 30% of COVID-19 survivors continue to experience a wide range of persistent symptoms for several weeks since their initial diagnosis. This condition is commonly referred to as post-acute sequelae of SARS-CoV-2 infection (PASC) or “long COVID.”
Even though multisystem inflammatory syndrome is the most common PASC syndrome in adults and children, a wide range of other symptoms, including sleep difficulties, persistent fatigue, type 1 diabetes, and neurological disorders, have been reported. The incidence of these symptoms varies from one person to another based on their demographic and clinical characteristics.
Several studies have indicated the manifestation of multiple cardiovascular complications, such as arrhythmia, hypertension, acute myocardial infarction, thromboembolism, and cerebrovascular accidents, in individuals who have recovered from COVID-19. However, a limited number of studies have confirmed that severe COVID-19 leads to a high risk of cardiovascular diseases.
A recent Clinical Infectious Diseases journal study determines the relationship between COVID-19 severity and risk of subsequent cardiovascular events (CVEs) in a large cohort.
Study findings
A retrospective cohort study was performed using nationwide health insurance claims data of adults from the United States Health Verity Real-Time Insights and Evidence database. Increased COVID-19 severity was found to enhance the risk of developing subsequent CVEs among individuals without a cardiac history in previous years.
As compared to COVID-19 patients who required outpatient care, those who required hospital admission were more likely to experience CVEs. Among COVID-19 hospitalized patients, those admitted to the intensive care unit (ICU) were almost 80% more likely to develop CVEs than non-ICU hospitalized patients.
In fact, non-ICU hospitalized patients exhibited only a 28% possibility of experiencing CVEs thirty days after initial COVID-19 symptoms. Additionally, as compared to COVID-19 outpatients, hospitalized patients were more likely to be admitted for a CVE after recovering from COVID-19.
In younger adults, the incidence of cardiovascular sequelae was lower as compared to older adults. Aside from CVEs, other severe outcomes, such as thrombotic events and cerebrovascular accidents, were observed in patients who recovered from severe COVID-19. However, such observations were less likely in COVID-19 patients who required only outpatient care.
The study findings emphasize the importance of vaccination, as demonstrated by its ability to reduce severe disease. Similarly, prompt antiviral treatment of acute COVID-19 has been recommended, which would help reduce the possibility of transition to severe illness.
Both COVID-19 vaccination and timely therapeutic interventions would alleviate the risk of severe COVID-19 and subsequently decrease the possibility of experiencing CVEs.
The findings of the present study are consistent with previous research that has reported a higher incidence of myocarditis and pericarditis in patients who recovered from severe SARS-CoV-2 infection. Nevertheless, it was observed that elevated cardiovascular risk after acute infection may not be exclusive to COVID-19.
In fact, some other diseases that have been associated with an increased risk of long-term CVEs are influenza and pneumonia bacteremia. Additionally, 22-65% of sepsis survivors are at an increased risk of CVEs.
The underlying mechanism responsible for the increased risk of CVEs following SARS-CoV-2 infection has not been determined. SARS-CoV-2 infects cardiac myocytes through their interaction with the angiotensin-converting enzyme 2 (ACE-2) receptor, which might remain persistent; therefore, this interaction induces chronic inflammatory responses and subsequent tissue damage or fibrosis.
Another mechanism related to the development of CVEs following recovery from COVID-19 is an autoimmune response to cardiac antigens that causes delayed damage to cardiac tissues. Anti-heart antibodies also correlated with cardiovascular manifestation and COVID-19.
Viral toxicity is another possible mechanism that might cause long-term cardiac damage or thrombosis in vasculitis. However, in the future, more research is needed to confirm the mechanisms related to cardiac damage after SARS-CoV-2 infection.
Conclusions
Due to the lack of a COVID-19-negative control group, the authors failed to quantify the elevated risk of CVEs in COVID-19 patients. The unwanted inclusion of patients with a history of CVEs could have overestimated the result as well. The impact of vaccination status on the incidence of CVE was not studied.
Despite these limitations, the present study strongly emphasized that patients who recovered from severe COVID-19 were at a greater risk of developing CVEs. As compared to COVID-19 patients who required outpatient care, those who were admitted to the ICU were at a higher risk of experiencing CVEs.
The importance of COVID-19 vaccination in preventing severe infection was strongly emphasized in this study.
Journal reference:
Wiemken, L. T., McGrath, L. J., Andersen, K. M., et al. (2022). COVID-19 severity and risk of subsequent cardiovascular events. Clinical Infectious Diseases. doi:10.1093/cid/ciac661.
Disclosures:
The authors report no relevant financial disclosures.
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com.
Exercise performance during cardiac rehabilitation, scored with a novel index, can reliably predict CV event risk at 1 year, according to data from a single-center study.
“Participating in a cardiac rehabilitation program is essential to improving patients’ survival and quality of life following myocardial infarction or heart surgery and for patients with HF,” Ofir Koren, MD, FESC, an interventional cardiology fellow with the Cedars-Sinai Medical Center Smidt Heart Institute and a senior interventional cardiologist with Emek Medical Center in Afula, Israel, told Healio. “Our study supports previous evidence and emphasizes the importance of understanding the level of endurance required to promote improved outcomes by designing a simple-to-use formula that can guide physicians and physiotherapists toward a target-directed program.”
Data were derived from Naami R, et al. Clin Cardiol. 2022;doi:10.1002/clc.23890.
Koren and colleagues analyzed data from 486 adults who participated in at least 80% of sessions in a cardiac rehabilitation program between January 2018 and August 2021 at Emek Medical Center in Israel. The rehab program is a twice weekly, 3-month government-funded program; each session includes exercises on a treadmill, elliptical, bicycle and handcycle. Researchers assessed patient performance using a novel index, the “CR score,” which integrated duration, speed of work and workload conducted on each training device. Researchers then determined the optimal thresholds for a cumulative CR score and assessed the mortality rate among patients who developed a major adverse CV event and those who did not (controls).
The findings were published in Clinical Cardiology.
Major adverse CV events occurred in 5.5% of patients at 1 year; events were more common among those with prior cerebrovascular accident or transient ischemic attack (14.8% vs. 3.5%; P < .001). Age, sex, comorbidities, HF and medical treatment did not affect the outcome.
The median cumulative CR score of the study group was lower compared with controls (median, 595 vs. 3,500; P < .0001). A cumulative CR score of greater than 1,132 correlated with the outcome with 98.5% sensitivity and 99.6% specificity (95% CI, 0.9850.997; P < .0001). Patients older than age 55 years with a cumulative CR score of greater than 1,132 were deemed at highest risk for a major adverse CV event at 1 year, with an OR of 7.4 (95% CI, 2.84-18.42); Kaplan-Meier survival curve indicated that major adverse CV events at 1 year occurred much earlier among patients with a low CR score (log-rank P = .03).
The researchers noted that the CR score is a novel score that has not been validated on a large scale.
“These data may assist physicians and physiotherapists in tailoring a specific CR program with clear physical targets,” Koren, also a clinic lecturer at Technion University in Israel, told Healio. “We need a prospective study involving two groups randomly assigned to two therapeutic options — current CR practice and a CR program directed using our model.”
For more information:
Ofir Koren, MD, FESC,can be reached at ofir.koren@cshs.org; Twitter: @dr_ofir.
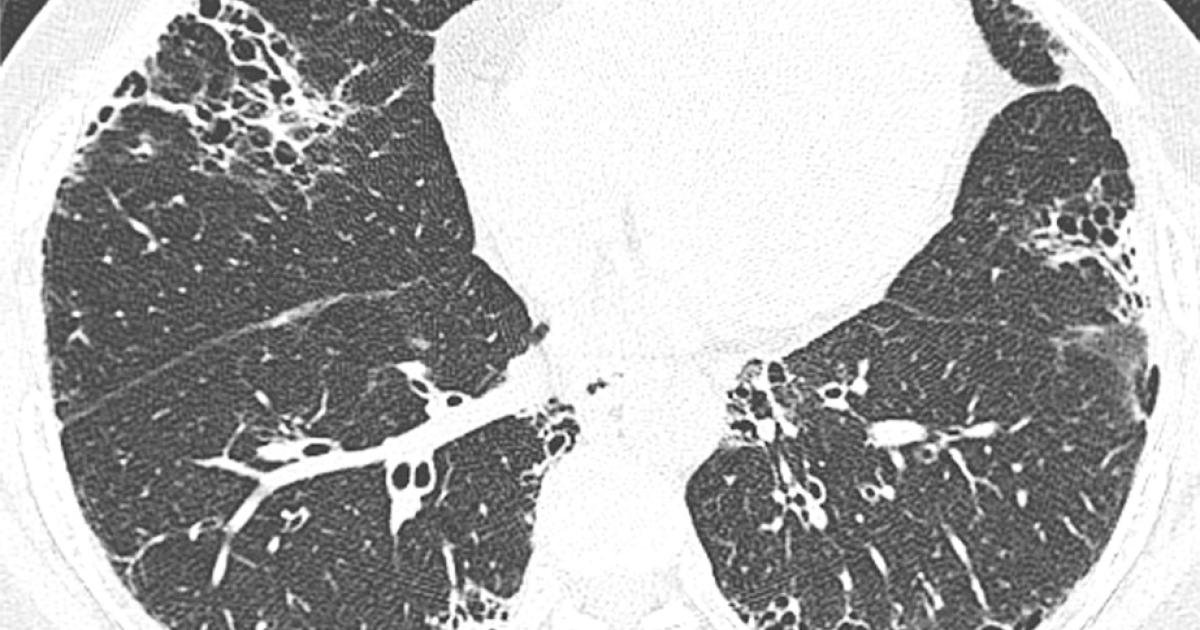
New research highlights key CT findings that radiologists should be aware of when interpreting the exams of patients with COVID pneumonia.
The paper details an analysis of 276 COVID patients and how their image findings correlated to their experiences with thromboembolic events. Corresponding author of the paper Mohd Ghadeeb, MD, from the Radiology Department at King Fahad Hospital in Saudi Arabia, and colleagues explained the importance and challenges involved in understanding COVID patients’ risks of clotting complications recently in Cureus:
“Thromboembolic manifestations have a wide spectrum and vary significantly among different patients. These include venous thromboembolic events, arterial events, and microvascular thrombosis,” the researchers wrote. “The diagnosis of venous thromboembolic events, including deep venous thrombosis and pulmonary embolism, can be challenging due to overlapping clinical and laboratory features.”
Ghadeeb and colleagues looked at the chest CT scans of patients admitted to their hospital with COVID pneumonia while also reviewing the patients’ electronic health records to single out anyone who had experienced a thromboembolic event. Out of these 276 admitted patients, 64 experienced thromboembolic events, 51 of whom were diagnosed with pulmonary embolism and 16 with deep vein thrombosis.
To the Editor: Jacobs et al. (May 19 issue)1 explored the association of several childhood risk factors (body-mass index [BMI], systolic blood pressure, total cholesterol level, triglyceride level, and smoking status) with vascular events in adulthood. They found that there was an association between childhood risk factors and cardiovascular events in midlife. However, neither albuminuria nor the estimated glomerular filtration rate (eGFR) was assessed. Albuminuria and a decreased eGFR are key risk factors for cardiovascular events and, together with BMI, systolic blood pressure, lipid levels, and smoking, are used in adults to assess cardiovascular risk. An elevated eGFR may indicate . . .
Four times since 1900, human civilization has suffered global catastrophes with extreme impacts: World War I (40 million killed), the 1918-19 influenza pandemic (40-50 million killed), World War II (40-50 million killed), and the COVID-19 pandemic (an economic impact in the trillions, and a 2020-21 death toll of 14.9 million, according to the World Health Organization).
These are the only events since the beginning of the 20th century that meet the United Nations’s definition of global catastrophic risk (GCR): a catastrophe global in impact that kills over 10 million people or causes over $10 trillion (2022 USD) in damage.
These reports, endorsed by United Nations Secretary-General António Guterres, make the case that the combined effects of disasters, economic vulnerabilities, and overtaxing of ecosystems are creating “a dangerous tendency for the world to tend toward the Global Collapse scenario. This scenario presents a world where planetary boundaries have been extensively crossed, and if GCR events have not already occurred or are in the process of occurring, then their likelihood of doing so in the future is extreme … and total societal collapse is a possibility.”
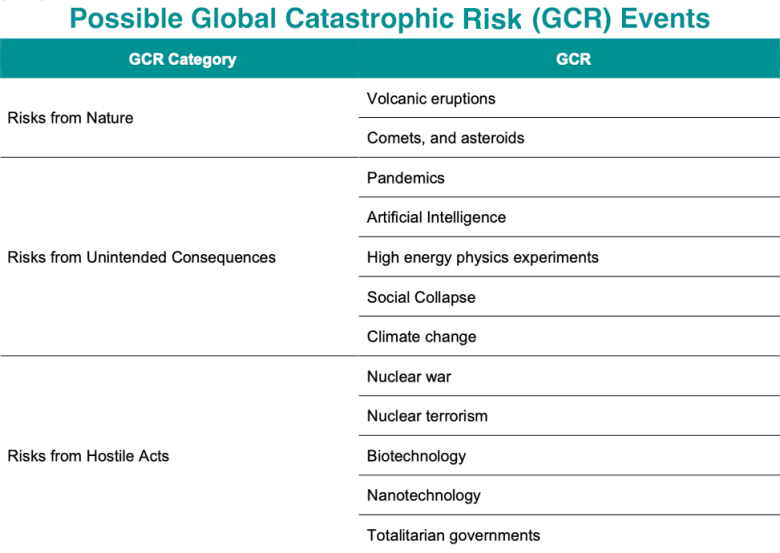
Human civilization has evolved during the Holocene Era, the stability of which is now threatened by human-caused climate change. As a result, global catastrophic risk events from climate change are growing increasingly likely, the U.N. May 2022 reports conclude. There are many other potential global catastrophic risk events, both natural and human-caused (Figure 2), posing serious risks and warranting humanity’s careful consideration. But the report cautions of “large uncertainty both for the likelihood of such events occurring and for their wider impact.” (Note that there is at least one other type of Global Catastrophic Risk event the report omits: an intense geomagnetic storm. A repeat of the massive 1859 Carrington Event geomagentic storm, which might crash the electrical grid for 130 million people in the U.S. for multiple years, could well be a global catastrophic risk event.)
Five types of GCR events with increasing likelihood in a warmer climate
1) Drought The most serious immediate global catastrophic risk event associated with climate change might well be a food-system shock caused by extreme droughts and floods hitting multiple major global grain-producing “breadbaskets” simultaneously. Such an event could lead to significant food prices spikes and result in mass starvation, war, and a severe global economic recession. This prospect exists in 2022-23, exacerbated by war and the COVID-19 pandemic.
The odds of such a food crisis will steadily increase as the climate warms. The author of this post presented one such scenario in an op-ed published in The Hill last year, and insurance giant Lloyds of London detailed another such scenario in a “food system shock” report issued in 2015. Lloyds gave uncomfortably high odds of such an event’s occurring—well over 0.5% per year, or more than a 14% chance over a 30-year period.
2) War In his frightening book Food or War, published in October 2019, science writer Julian Cribb documents 25 food conflicts that have led to famine, war, and the deaths of more than a million people – mostly caused by drought. For example, China’s drought and famine of 1630-31 led to a revolt that resulted in the collapse of the Ming Dynasty. Another drought in China in the mid-nineteenth century led to the Taiping rebellion, which claimed 20-30 million lives.
Since 1960, Cribb says, 40-60% of armed conflicts have been linked to resource scarcity, and 80% of major armed conflicts occurred in vulnerable dry ecosystems. Hungry people are not peaceful people, Cribb argues, and ranks South Asia – India, Pakistan, Bangladesh, and Sri Lanka – as being at the most risk of future food/water availability conflicts. In particular, nuclear powers India and Pakistan have a long history of conflict, so climate change can be expected to increase the risk of nuclear war between them. A “limited” nuclear war between India and Pakistan, 100 bombs dropped on cities. would be capable of triggering a global “nuclear winter” with a death toll up to two billion, Helfand (2013) estimated.
3) Sea-level rise, combined with land subsidence During the coming decades, it will be very difficult to avoid a global catastrophic risk event from sea-level rise, when combined with coastal subsidence from groundwater pumping, loss of river sedimentation from flood-control structures, and other human-caused effects: A moderate global warming scenario (RCP 4.5) will put $7.9-12.7 trillion dollars of global coastal assets at risk of flooding by 2100, according to a 2020 study by Kirezci et al., “Projections of global-scale extreme sea levels and resulting episodic coastal flooding over the 21st Century.” While this study did not take into account assets that inevitably will be protected by new coastal defenses to be erected, neither did it consider the indirect costs of sea-level rise from increased storm surge damage, mass migration away from the coast, salinification of fresh water supplies, and many other factors. A 2019 report by the Global Commission on Adaptation estimated that sea level rise will lead to damages of more than $1 trillion per year by 2050.
Furthermore, sea-level rise, combined with other stressors, might bring about megacity collapse – a frightening possibility with infrastructure destruction, salinification of fresh water resources, and a real estate collapse potentially combining to create a mass exodus of people, reducing the tax base of the city to the point that it can no longer provide basic services. The collapse of even one megacity might have severe impacts on the global economy, creating increased chances of a cascade of global catastrophic risk events. One megacity potentially at risk of this fate is the capital of Indonesia, Jakarta, with a population of 10 million). Land subsidence (up to two inches per year) and sea-level rise (about 1/8 inch per year) are so high in Jakarta that Indonesia currently is constructing a new capital city in Borneo. Plans call for moving 8,000 civil servants there in 2024, and eventually move 1.5 million workers from Jakarta to the new capital by 2045.
4) Pandemics As Earth’s climate warms, wild animals will be forced to relocate their habitats and increasingly enter regions with large human populations. This development will dramatically increase the risk of a jump of viruses from animals to humans that could lead to a pandemic, according to a 2022 paper by Carlson et al. in Nature, “Climate change increases cross-species viral transmission risk.”Bats are the type of animal of most concern.
Note that in the case of the 1918-19 influenza GCR event, a separate GCR event helped trigger it: WWI, because of the mass movement of troops that spread the disease. The U.N. reports emphasize that one GCR event can trigger other GCR events, with climate change acting as a threat multiplier.
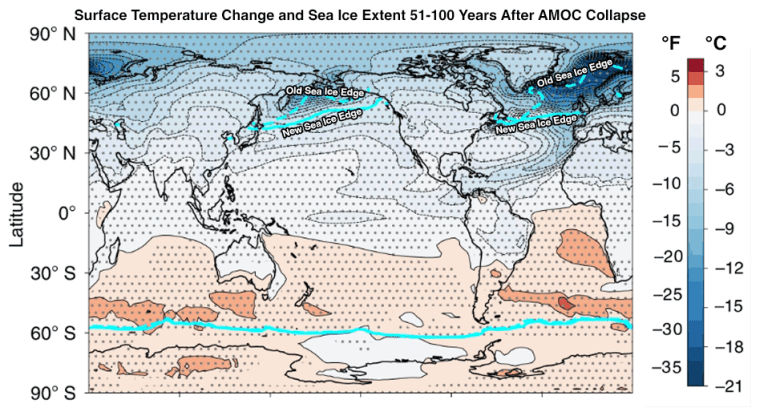
Figure 3. Predicted change in surface temperature 51-100 years after a failure of the Atlantic Meridional Overturning Circulation. Catastrophic cooling is predicted to affect Northern Europe, the edge of arctic sea ice reach northern France, and temperatures in the U.S. fall 1-2 degrees Celsius (1.8-3.6°F). Sea ice edges are shown in bright blue; the sea ice edge would remain virtually unchanged in the Southern Hemisphere, but advance significantly equatorward in the Northern Hemisphere, reaching northern France. (Image credit: modified from Orihuela-Pinto et al., 2022, Interbasin and interhemispheric impacts of a collapsed Atlantic Overturning Circulation, Nature Climate Change, https://doi.org/10.1038/s41558-022-01380-y)
5) Ocean current changes Increased precipitation and glacial meltwater from global warming could flood the North Atlantic with enough fresh water to slow down or even halt the Atlantic Meridional Overturning Circulation (AMOC), the ocean current system that transports warm, salty water from the tropics to the North Atlantic and sends cold water to the south along the ocean floor. If the AMOC were to shut down, the Gulf Stream would no longer pump warm, tropical water to the North Atlantic. Average temperatures would cool in Europe by three degrees Celsius (5.4°F) or more in just a few years – not enough to trigger a full-fledged ice age, but enough cooling to bring snows in June and killing frosts in July and August, as occurred in the famed 1816 “year without a summer” caused by the eruption of Mt. Tambora. In addition, shifts in the jet stream pattern might bring about a more La Niña-like climate, causing an increase in drought to much of the Northern Hemisphere, greatly straining global food and water supplies.
A study published in August 2021 looked at eight independent measures of the AMOC, and found that all eight showed early warning signs that the ocean current system may be nearing collapse. “The AMOC may have evolved from relatively stable conditions to a point close to a critical transition,” the authors wrote.
Figure 4. A pteropod shell is shown dissolving over time in seawater with a lower pH. When carbon dioxide is absorbed by the ocean from the atmosphere, the chemistry of the seawater is changed. (image credit: NOAA)
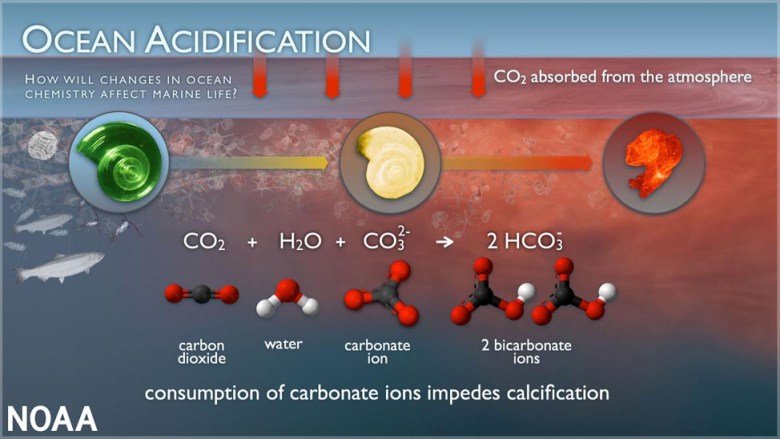
6) Ocean acidification The increased carbon dioxide in the atmosphere is partially absorbed by the oceans, making them more acidic. Since pre-industrial times, the pH of surface ocean waters has fallen by 0.1 pH units, to 8.1 – approximately a 30 percent increase in acidity. Increased acidity is harmful to a wide variety of marine life, and acidic oceans have been linked to several of Earth’s five major extinction events through geologic time.
Under a business-as-usual emission scenario, continued emissions of carbon dioxide could make ocean pH around 7.8 by 2100. The last time the ocean pH was this low was during the middle Miocene, 14-17 million years ago. The Earth was several degrees warmer and a major extinction event was occurring.
7) A punishing surprise In 2004, Harvard climate scientists Paul Epstein and James McCarthy conclude in a paper titled “Assessing Climate Stability” that: “We are already observing signs of instability within the climate system. There is no assurance that the rate of greenhouse gas buildup will not force the system to oscillate erratically and yield significant and punishing surprises.” Hurricane Sandy of 2012 was an example of such a punishing surprise, and climate change will increasingly bring low-probability, high impact weather events – “black swan” events – that no one anticipated. As the late climate scientist Wally Broecker once said, “Climate is an angry beast, and we are poking at it with sticks.”
Figure 5. An 18 km-high volcanic plume from one of a series of explosive eruptions of Mount Pinatubo on June 12, 1991, viewed from Clark Air Base. Three days later, the main eruption produced a plume that rose nearly 40 km, penetrating well into the stratosphere. Pinatubo’s sulfur emissions cooled the Earth by about 0.5 degree Celsius (0.9°F) for 1-2 years. (Photograph by David H. Harlow, USGS.)
Volcanic eruptions: A decreasing likelihood in a warming climate
Climate change can also be expected to reduce the likelihood of one type of global catastrophic risk event: the impacts of a massive volcanic eruption. A magnitude-seven “super-colossal” eruption with a Volcanic Explosivity Index of seven (VEI 7) occurred in 1815, when the Indonesian volcano Tambora erupted. (The Volcanic Explosivity Index is a logarithmic scale like the Richter scale used to rate earthquakes, so a magnitude 7 eruption would eject ten times more material than a magnitude 6 eruptions like that of Mt. Pinatubo in the Philippines in 1991.)
The sulfur pumped by Tambora’s eruption into the stratosphere dimmed sunlight so extensively that Northern Hemisphere temperatures fell by about 0.4-0.7 degree Celsius (0.7-1.0°F) for 1-2 years afterward. The result: the famed Year Without a Summer in 1816. Killing frosts and snow storms in May and June 1816 in Eastern Canada and New England caused widespread crop failures, and lake and river ice were observed as far south as Pennsylvania in July and August. Famine and food shortages rocked the world.
Verosub (2011) estimated that future eruptions capable of causing “volcanic winter” effects severe enough to depress global temperatures and trigger widespread crop failures for one to two years afterwards should occur about once every 200-300 years, which translates to a 10-14% chance over a 30-year period. An eruption today like the Tambora event of 1815 would challenge global food supplies already stretched thin by rising population, decreased water availability, and conversion of cropland to grow biofuels.
However, society’s vulnerability to major volcanic eruptions is less than it was, since the globe has warmed significantly in the past 200 years. The famines from the eruption of 1815 occurred during the Little Ice Age, when global temperatures were about 0.9 degree Celsius (1.6°F) cooler than today, so crop failures from a Tambora-scale eruption would be less widespread than is the case with current global temperatures. Fifty years from now, when global temperatures may be another 0.5 degree Celsius warmer, a magnitude seven eruption should be able to cool the climate only to 1980s levels. However, severe impacts to food supplies still would result, since major volcanic eruptions cause significant drought. (To illustrate, in the wake of the 1991 climate-cooling VEI 6 eruption of the Philippines’ Mt. Pinatubo, land areas of the globe in 1992 experienced their highest levels of drought for any year of the 1950-2000 period.)
Unfortunately, the future risk of a volcanic global catastrophic risk event may be increasing from causes unrelated to climate change, because of the increasing amount of critical infrastructure being located next to seven known volcanic hot spots, argued Mani et al. in a 2021 paper, “Global catastrophic risk from lower magnitude volcanic eruptions.” For example, a future VEI 6 eruption of Washington’s Mount Rainier could cost more than $7 trillion over a 5-year period because of air traffic disruptions; similarly, a VEI 6 eruption of Indonesia’s Mount Merapi could cost more than $2.5 trillion.
Commentary
Complex systems like human cultures are resilient, but are also chaotic and unstable, and vulnerable to sudden collapse when multiple shocks occur. Jared Diamond’s provocative 2005 book, Collapse: How Societies Choose to Fail or Succeed, described flourishing civilizations or cultures that eventually collapsed, like the Greenland Norse, Maya, Anasazi, and Easter Islanders. Environmental problems like deforestation, soil problems, and water availability were shown to be a key factor in many of these collapses.
“One of the main lessons to be learned from the collapses of the Maya, Anasazi, Easter Islanders, and those other past societies,” Diamond wrote, “is that a society’s steep decline may begin only a decade or two after the society reaches its peak numbers, wealth, and power. … The reason is simple: maximum population, wealth, resource consumption, and waste production mean maximum environmental impact, approaching the limit where impact outstrips resources.”
Some of Diamond’s conclusions, however, have been challenged by anthropologists. For example, the 2010 book, Questioning Collapse: Human Resilience, Ecological Vulnerability, and the Aftermath of Empire, argued that societies are resilient and have a long history of adapting to, and recovering from, climate change-induced collapses. But a 2021 paper by Beard et al., “Assessing Climate Change’s Contribution to Global Catastrophic Risk,” argued, pointed to “reasons to be skeptical that such resilience can be easily extrapolated into the future. First, the relatively stable context of the Holocene, with well-functioning, resilient ecosystems, has greatly assisted recovery, while anthropogenic climate change is more rapid, pervasive, global, and severe.”
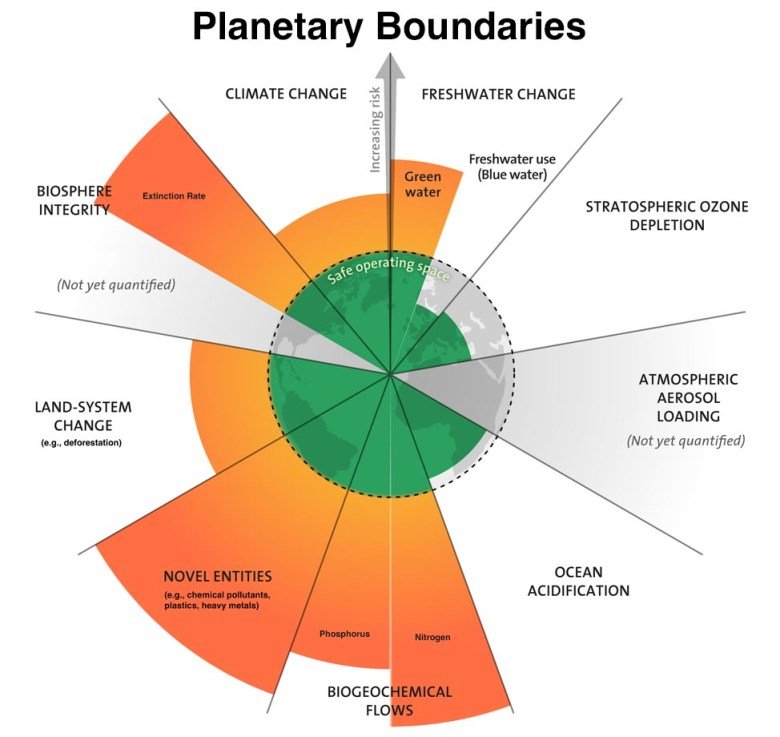
To paraphrase, one can think of the nine planetary boundaries as credit cards, six of those nine credit cards charged to the hilt to develop civilization as it now exists. But Mother Nature is an unforgiving lender, and there is precious little credit available to help avoid a cascade of interconnected global catastrophic risk events that might send human society into total collapse, if society unwisely continues its business-as-usual approach.
Avoiding climate change-induced global catastrophic risk events is of urgent importance, and the UN report is filled with promising approaches that can help. For example, it explains how systemic risk in food systems from rainfall variability in the Middle East can be reduced using traditional and indigenous dryland management practices involving rotational grazing and access to reserves in the dry season. More generally, the encouraging clean energy revolution now under way globally needs to be accelerated. And humanity must do its utmost to pay back the loans taken from the Bank of Gaia, stop burning fossil fuels and polluting the environment, and restoring degraded ecosystems. If we do not, the planet that sustains us will no longer be able to.
Bob Henson contributed to this post.
Website visitors can comment on “Eye on the Storm” posts (see comments policy below). Sign up to receive notices of new postings here.
If you’ve ever applied for a loan or business insurance, you’ve had to check a box that asked whether you had a Business Continuity Plan in place. Many applicants tend to mindlessly check yes, even if they don’t have an actual plan in place.
Continuity plan checks are part of loan and insurance applications
getty
That is not a good idea. There’s a reason why these institutions ask for a Business Continuity Plan. And it’s not to annoy you or give you unnecessary work. They are looking to minimize risk for you and for their institution. Many are required by law to have a Business Continuity plan in place themselves.
A Business Continuity Plan is a contingency plan that provides direction about how to keep the business in operation if something unexpected were to happen. Loan and insurance applications aside, having a plan forms part of a solid business strategy particularly during times of uncertainty.
Research indicates that close to 90% of businesses with a Business Continuity Plan reported having reduced disruptions, improved resilience, and faster recovery from disruptions. So there are a number of statistically proven benefits to having a Business Continuity Plan.
Disruptions can be natural or they can be manmade. Some of the most common disruptions – an unexpected death, divorce, distress, disability, or disagreement – will affect 1 in 2 businesses. Any one of these can have a devastating impact, particularly on a smaller business.
Business Continuity Planning helps businesses confidently respond to unplanned events.
getty
How devastating? The average disruption will cost the business about $81,000. And still 25% of businesses will shut down entirely. That’s pretty devastating for a business without the resources to buffer the impact.
Business interruption insurance may help but only in cases where ‘a covered event causes physical damage that results in losses’. Many of the most common disruptions would therefore not be eligible for a business interruption payout as many found out during the pandemic. Check the policy or speak with your broker.
The responsibility for protecting people, profits, and the company’s growth from unplanned events is an internal job. This type of risk management and risk mitigation cannot be outsourced or delegated.
Business Continuity Plans typically include information on:
Whom to contact in and out of the organization. This of course includes employees, but also customers, suppliers and key stakeholders, etc.
Key documents. It’s essential to record where to find documents like lease, mortgage, key contracts, along with the person(s) with access.
Financial matters. This is usually an important one because even during a disruption the business needs to be able to continue to pay and be paid. Basics include information on location of accounts and names of signatories to the accounts – i.e. who has access.
Operational workarounds. What are the key tasks that keep the business running? How are they performed now and how can they continue to be performed if the current way of working were for some reason impacted now? There’s a lot of talk about cybersecurity and cyber threats. If something were to happen that prevented the business from operating in its usual way, what workarounds will allow it to continue?
Thinking through and documenting this information ahead of time minimizes response times during a disruption. This level of foresight also reduces the number of decisions that would need to be made during a disruption when emotions are heightened and the business may be losing money.
Continuity planning allows business leaders to focus on making the right strategic decisions to navigate the disruption instead of expending energy on day to day operational decisions in the heat of the moment.
Documenting these areas ensures that the relevant information is at the business’ fingertips during a disruption when the most important thing needed is readily accessible information. Once this information is documented, it’s essential that the people tasked with responding are informed and trained.
Running a business comes with inherent risks. Business leaders taking on this risk own it by taking steps to proactively insulate their growth and operations from unpredictable and unplanned events. Having a business continuity plan is one of those steps.
Lam L, et al. Abstract OS006. Presented at: International Liver Congress; June 22-26, 2022; London (hybrid meeting).
Disclosures:
Healio was unable to confirm relevant financial disclosures at the time of publication.
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com.
LONDON — Direct-acting antiviral treatment correlated with a decreased risk for cardiovascular outcomes among patients with hepatitis C virus and advanced fibrosis but an increased risk for arrhythmias and conduction disorders.
“Several studies have revealed that hepatitis C virus can induce chronic inflammation and immune dysregulation, and this immune dysregulation and chronic inflammation explained the development of extrahepatic manifestations in chronic hepatitis C patients, including cardiovascular disease,” Laurent Lam, MD, a physician and doctoral researcher at the Pierre Louis Institute of Epidemiology and Public Health at Sorbonne University in Paris, told attendees at the International Liver Congress. “Few data are available regarding the long-term impact of DAAs on the occurrence of non-liver events.”
Using the prospective ANRS CO22 HEPATHER cohort, which derived individual data from the French National Health Insurance Database, Lam and colleagues analyzed 8,148 patients with chronic HCV between August 2012 and December 2015 for cardiovascular events and cancer incidence. The primary outcome was the association between DAA use and extrahepatic events.
Among 22,326 and 12,905 person-years of DAA and no DAA exposure, analysis showed DAA exposure correlated with a reduced risk for peripheral arterial disease (HR = 0.54; 95% CI, 0.33-0.89), an overall beneficial effect on cardiovascular among patients with HCV/advanced fibrosis (adjusted HR = 0.58; 95% CI, 0.42-0.79) and an increased risk for arrhythmias and conduction disorders (HR = 1.46; 95% CI, 1.04-2.04).
Lam and colleagues observed no association between DAA use and extrahepatic cancer (HR = 1.23; 95% CI, 0.5-3.03).
“Direct-acting antiviral exposure reduced the risk for peripheral arterial disease, overall cardiovascular events and increased risk for arrhythmias and conduction disorders,” Lam concluded. “Direct acting antivirals are not associated with extrahepatic cancer development or reduction in our study.”
1. In this cohort study, among 16 374 Swedish adult patients with primary hyperparathyroidism, the risk hip fracture was increased by 51%, and risk of cardiovascular events increased by 45% compared to matched healthy participants.
2. Parathyroidectomy was associated with a reduced risk of any fracture, hip fracture, cardiovascular events and death.
Evidence Rating Level: 2 (Good)
Study Rundown: Primary hyperparathyroidism (pHPT) is an endocrine disorder in which individuals have an elevated serum calcium combined with a normal or high blood level of parathyroid hormone. Known concerns of pHPT include increased bone loss and an elevated risk of fractures at sites including the spine, wrist, ribs and pelvis. As such, this retrospective cohort study investigated whether untreated pHPT was associated with an increased risk of fractures and cardiovascular events (CVEs) in comparison with the risk of a sex, age and country-matched control group and whether parathyroidectomy was associated with a reduction in these outcomes. The study included patients who were diagnosed with pHPT at hospitals in Sweden between 2006 to 2017. The primary outcomes were fractures, CVEs, and death. A total of 16 374 patients with pHPT were identified with a mean age of 67.5 years. Compared with the control group, the pHPT group was found to have a higher risk of any fracture by 39%, hip fracture by 51%, CVEs 45% and death 72%. Parathyroidectomy was associated with a reduced risk of any fracture by 17% and death by 59%. A major strength of this study was that in terms of the number of patients with untreated pHPT and multiple observed outcomes, it is the largest analysis performed thus far. As a result of the observational design however, a limitation to this study is that it could not establish causality, although the time-dependent analysis suggested an association between parathyroidectomy and reduced risk of fractures, CVEs and death.
In-Depth [retrospective cohort]: This study investigated whether primary hyperparathyroidism (pHPT) was associated with an increased risk of fractures, CVEs and mortality, compared to the risk of a sex, age and country-matched control group. Data was collected from patients diagnosed with pHPT at hospitals in Sweden between July 1, 2006 to December 31, 2017. Each patient was matched with 10 control individuals from the general population. A total of 16 374 patients with pHPT were identified (mean SD age, 67.5 [12.9] years; 12806 women [78.2%]), with 163 740 control individuals. The median follow-up time for the pHPT group was 1.15 (.040-4.06) years and for the control it was 4.62 (2.08-7.51) years. Patients with pHPT had significantly higher risks of any fracture (unadjusted HR, 1.39; 95% CI, 1.31-1.48), major osteoporotic fracture (unadjusted HR, 1.43; 95% CI, 1.33-1.54), hip fracture (unadjusted HR, 1.51; 95% CI, 1.35-1.70), and injurious fall (unadjusted HR, 1.51; 95% CI, 1.42-1.60) compared with those in the control group. The risk of fractures was significantly increased at the following sites: wrist (unadjusted HR, 1.34; 95 CI, 1.18-1.52), upper arm (unadjusted HR, 1.46; 95% CI, 1.25-1.71) and lower leg (unadjusted HR, 1.31; 95% CI, 1.12-1.54). The risk of any CVE for patients with pHPT was increased (unadjusted HR, 1.45; 95% CI, 1.34-1.57), as well as the risk for acute myocardial infarction (unadjusted HR, 1.39; 95% CI, 1.24-1.56) and ischemic stroke (unadjusted HR, 1.51; 95%CI, 1.36-1.68). The risk of death (unadjusted HR, 1.72; 95% CI, 1.65-1.80) was also increased in higher in patients with pHPT compared to the control group. There was a substantial increase in the risk of kidney stones, almost 4 times higher in patients with pHPT (unadjusted HR, 3.65; 95% CI, 3.27-4.08) than in control individuals. Of the 16 374 patients with pHPT, 6934 (42.3%) underwent a parathyroidectomy. While using the Poisson regression model to study the pHPT group separately, parathyroidectomy was found to be associated with a reduced risk of hip fracture (HR, 0.78; 95% CI, 0.61-0.98), any fracture (HR, 0.83; 95% CI, 0.75-0.93), injurious fall (HR, 0.83; 95% CI, 0.74-0.92), CVE (HR, 0.84; 95% CI, 0.73-0.97), and death (HR, 0.59; 95% CI, 0.53-0.65).
Testosterone replacement therapy appears safe in the short-to-medium term to treat a condition caused by deficiency of the male sex hormone, according to the most comprehensive analysis of the treatment to date, published in The Lancet Healthy Longevity journal.
The findings suggest that men given testosterone to treat hypogonadism are at no greater risk of heart attack, stroke, and other cardiovascular events in the short-to-medium term than men who do not receive testosterone treatment.
Testosterone replacement therapy is the standard treatment for hypogonadism, which can cause sexual dysfunction, weakening of bones and muscles, and reduced quality of life. Risk factors for the condition include aging (as testosterone levels decline with age), obesity (BMI of 30 kg/m2 or above), and diabetes.
Despite being widely used, the cardiovascular safety of testosterone treatment has until now remained unclear due to inconsistent findings. This is because most previous clinical studies have relied on aggregate data, rather than individual participant data and have not published details of individual adverse events.
Prescribing of testosterone for hypogonadism is increasing globally, but conflicting messages about its safety may have led to many patients not receiving the treatment. Ongoing studies should help to determine the longer-term safety of testosterone but, in the meantime, our results provide much-needed reassurance about its short-to-medium term safety. Our findings could have important implications for the treatment of men with hypogonadism worldwide.”
Jemma Hudson, Study Lead Author, University of Aberdeen
The authors conducted a systematic review identifying 35 eligible clinical trials published since 1992, of which 17 provided individual participant data. A blinded analysis by two independent clinicians enabled the classification of every cardiovascular event, allowing for a more robust analysis of the cardiovascular safety of testosterone treatment.
A meta-analysis using individual participant data from 17 studies and a further meta-analysis integrating these data with the aggregate data provided by the 18 trials that did not provide individual participant data were performed.
Among the 17 trials with individual patient data, 1,750 participants received testosterone and 1,681 were given a placebo. The average length of testosterone treatment was 9.5 months. The average age of participants was 65 years, and most were white and did not smoke. Participants’ average BMI was 30 kg/m2, which is considered obese.
A meta-analysis showed there were 120/1,601 (7.5%) cardiovascular events in the testosterone group and 110/1,519 (7.2%) in the placebo group across 13 trials that provided this information. Patient age, smoking or diabetes status did not affect cardiovascular risk. Similarly, there was no significant difference in mortality rate between the testosterone group (6/1,621 deaths, 0.4%) and the placebo group (12/1,537 deaths, 0.8%) across the 14 trials that provided individual patient data on mortality, but only limited data were available.
The researchers also found that testosterone significantly reduced serum total cholesterol, high-density lipoprotein (HDL), and triglycerides compared with placebo. However, there were no significant differences in serum low-density lipoprotein (LDL), blood pressure, glycaemic parameters, diabetes incidence, and prostate adverse outcomes between the testosterone and placebo groups.
The meta-analysis that integrated individual participant data with aggregate data showed similar results.
The authors acknowledge some limitations to their study. There was little available data evaluating the cardiovascular safety of testosterone treatment beyond 12 months, and the very small number of deaths recorded during testosterone trials hampered the authors’ ability to analyze why they occurred.
However, the longer-term safety of testosterone treatment is currently being investigated in another clinical trial. While the meta-analysis of aggregate data showed similar results to the one involving individual patient data only, it cannot be ruled out with certainty that a high number of unreported cardiovascular events in the trials that did not provide individual participant data could alter the current conclusions.
Source:
Journal reference:
Hudson, J., et al. (2022) Adverse cardiovascular events and mortality in men during testosterone treatment: an individual patient and aggregate data meta-analysis. The Lancet Healthy Longevity. doi.org/10.1016/S2666-7568(22)00096-4